
Plancher KD, Voigt C, Bernstein DN, Briggs KK, Petterson SC. Return to Sport in Middle-aged and Older Athletes After Unicompartmental Knee Arthroplasty at a Mean 10-Year Follow-up: Radiographic and Clinical Outcomes. Am J Sports Med. 2023 Jun;51(7):1799-1807. doi: 10.1177/03635465231163859. Epub 2023 Apr 24. PMID: 37092711.
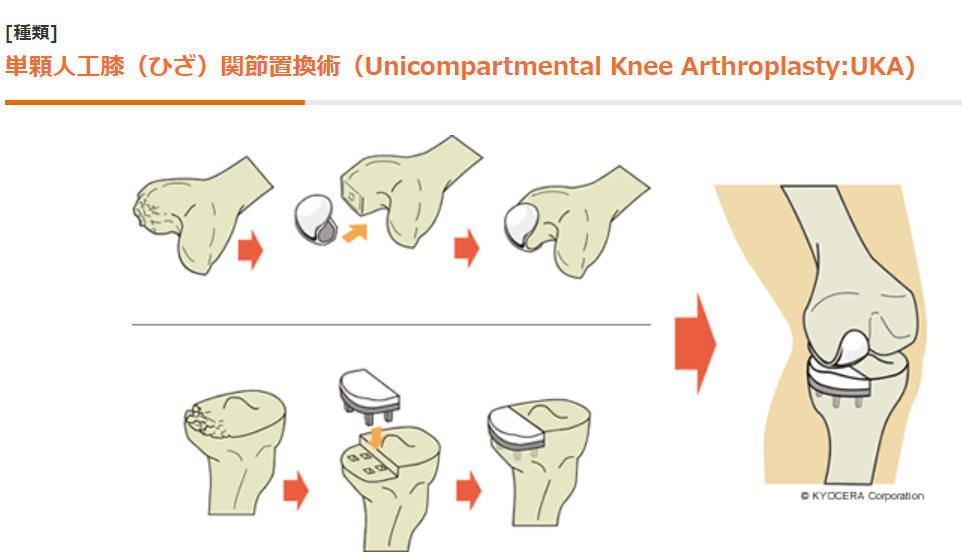
そもそもUKAとは?
人工膝関節単顆置換術 膝の内側か外側のどちらかの関節面のみを人工関節に置換すること
日本人は内側の軟骨摩耗(変形)が多く外側が無事で有ることが多いので
可動域保たれていたり十字靱帯が保たれているならこちらを選択することも多い
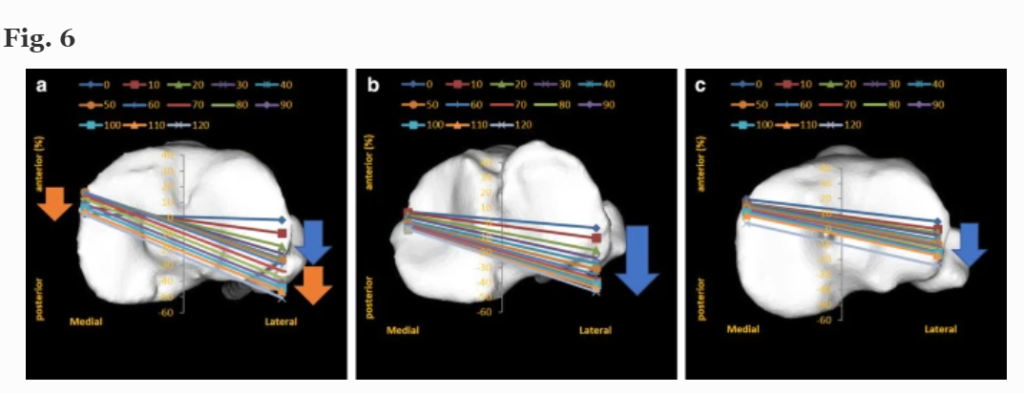
そして膝可動時の運動(内側を軸にして大腿骨外側が屈曲とともに後ろに引き下がる)も健常膝と類似しているのである
※上画像は屈曲時と関節面の内外側接触位置をなぞった図
左が健常膝、真ん中がUKA、右が前・後十字靱帯残した人工膝関節置換膝(BCR-TKA)
BCR-TKAは引き下がりが足りず、内側が軸とならず一緒に引き下がっている
Kono K, Inui H, Tomita T, Yamazaki T, Taketomi S, Tanaka S. Bicruciate-retaining total knee arthroplasty reproduces in vivo kinematics of normal knees to a lower extent than unicompartmental knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2020 Sep;28(9):3007-3015. doi: 10.1007/s00167-019-05754-2. Epub 2019 Oct 22. PMID: 31641811.
そもそものUKA後の術後2年以降のスポーツ復帰率(しかもサッカー等負担が大きいもの)は90%以上
Radhakrishnan GT, Magan A, Kayani B, Asokan A, Ronca F, Haddad FS. Return to Sport After Unicompartmental Knee Arthroplasty: A Systematic Review and Meta-analysis. Orthop J Sports Med. 2022 Mar 16;10(3):23259671221079285. doi: 10.1177/23259671221079285. PMID: 35321207; PMCID: PMC8935568.
理由は不明だが術後スポーツ制限しなくても良いと患者に伝えると54.2%はスポーツに復帰した(平均観察期間20.2ヵ月)
もしかしたらUKAスポーツ復帰を妨げている最たる理由は医師の都合なのかもしれない
Kleeblad LJ, Strickland SM, Nwachukwu BU, Kerkhoffs GMMJ, Pearle AD. Satisfaction with return to sports after unicompartmental knee arthroplasty and what type of sports are patients doing. Knee. 2020 Mar;27(2):509-517. doi: 10.1016/j.knee.2019.11.011. Epub 2020 Jan 8. PMID: 31926669.
活動度高い内側膝OAにはAKO(骨切り術)活動度低いものはUKAというのが定説であったが、インプラント耐久性も向上しており、その定説が崩れるかもしれない。
(ただしAKOの方がアライメント矯正も行えるので、汎用性はUKAより高いと思われる(私見))
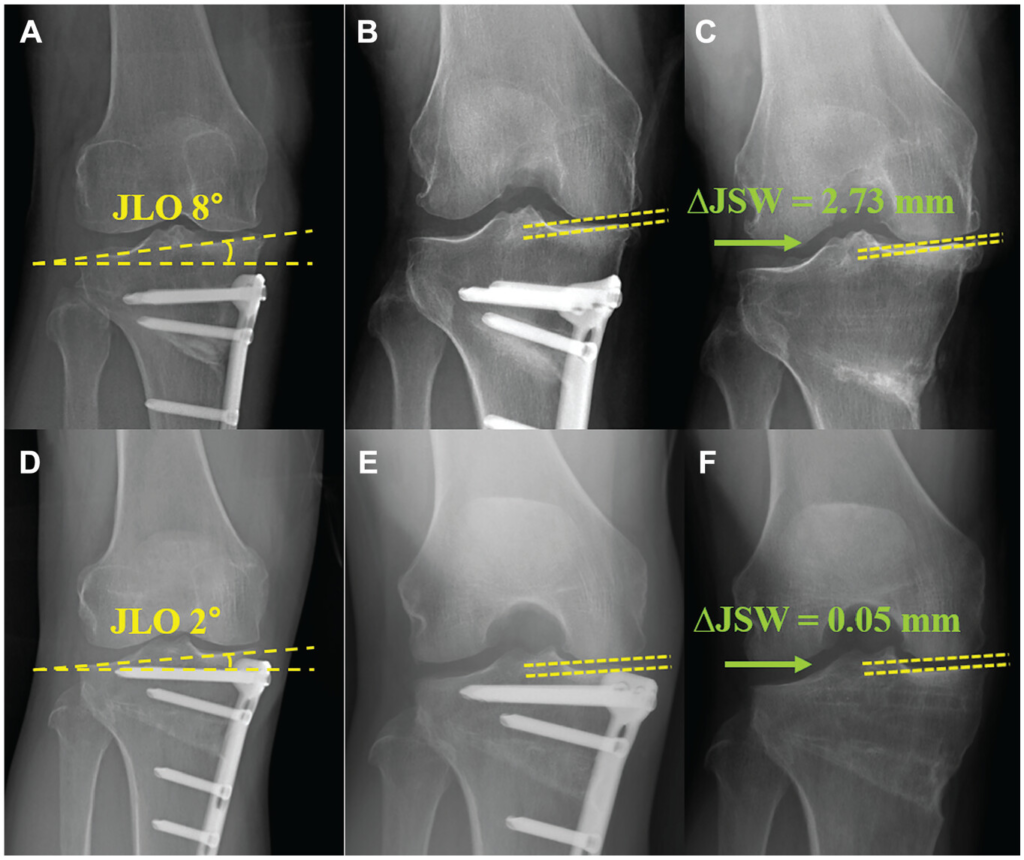
 術後全下肢長尺撮影がなされていないため下肢全体の形態が分からない
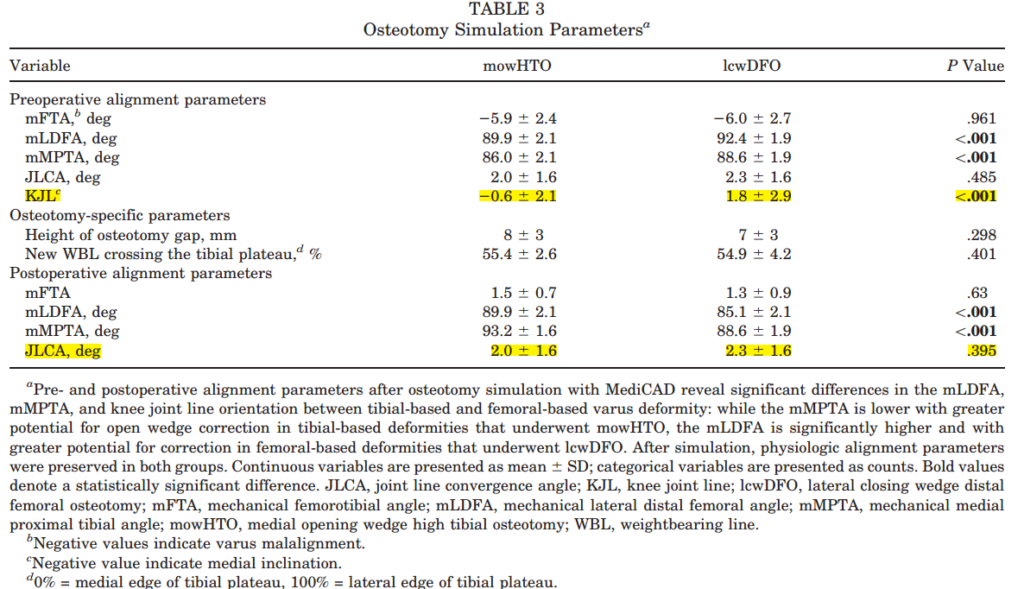
術後全下肢長尺撮影がなされていないため下肢全体の形態が分からない そもそも母集団のベースが違う(MPTA小さいのはMOWHTO、mLDFA大きいのはLCWDFO)なので真の比較研究ではないのでは?
そもそも母集団のベースが違う(MPTA小さいのはMOWHTO、mLDFA大きいのはLCWDFO)なので真の比較研究ではないのでは?